What are Children's Therapeutic Supports and Services?
Children's Therapeutic Supports and Services, as described in the MHCP manual here, are:
Psychotherapy to address a child's underlying mental health disorder;
Skills Training to teach/reinforce behavioral and psychosocial skills developed and taught in psychotherapy.
Skills training facilitates the acquisition and retention of behavioral, functional, or psychosocial skills that are medically necessary to rehabilitate the child to an age-appropriate developmental trajectory that has been disrupted by a diagnosed mental health disorder. Skills training may also be delivered to help the child or youth to self-monitor, compensate for, cope with, counteract, or replace skill deficits or maladaptive skills acquired during the course of a mental illness.
Behavioral Aide services to practice, repeat, reintroduce and master these skills. At this time, Accend does not provide Behavioral Aide services. All CTSS services are provided by MH Professionals or MH pracitioners.
CTSS also includes Crisis Assistance services, described in more detail below to help the child, the child’s family and all providers of services to the child to successfully prepare for and prevent or respond to potential crises.
Children and young adults up to age 21 are eligible for CTSS. Generally, we would recommend ARMHS for young adults.
To be eligible for CTSS, recipients must:
- be under 21 years old
- have a diagnostic assessment current within the previous 365 days that identifies a primary diagnosis of an emotional disturbance or mental illness for which treatment with CTSS is medically necessary to:
- restore a child or adolescent to an age-appropriate developmental trajectory that had been disrupted by a psychiatric illness; or
- enable the child to self-monitor, compensate for, cope with, counteract, or replace psychosocial skills, deficits or maladaptive skills acquired over the course of a psychiatric illness.
Before CTSS services can begin, we must
- complete the DA or review a recent external DA;
- complete the initial CASII or ECSII, service intensity instruments that identify a recommended level of care; and
- complete and obtain the parent or guardian's signature on the Individual Treatment Plan.
Initiating Services and Start Date
Once all of the above are complete and services have begun, mark the child's status as active.
While assessment and planning is occurring, the status should be Initiating.
Assessment and planning in CTSS is a child- and family-centered process that begins with the DA, but that continues with learning a child's current strengths. What does the child do well? Where is he or she succeeding? With whom, and in what environments are the child's functioning and behavior most optimal?
Identifying problems and possible delays in development, behavior and functioning is next. As with strengths, what differences exist in different environments?
Identifying both strengths and deficits, and environmental differences in behavior can give us insight into underlying causes for a child's behavior, and influences on functioning, and inform the treatment plan.
Functional Behavior Assessment
While not required for CTSS services by statute, a Functional Behavior Assessment is a useful tool. The Functional Behavior Assessment for CTSS Skills can be used for identifying the desired behaviors CTSS treatment seeks to increase as well as the functions of maladaptive/undesired behavior and the replacment behaviors that can be taught/reinforced to repace undesired behavior.
Standardized Outcome Measures for Children’s Mental Health
CASII and ECSII
While Minnesota Department of Human Services (DHS) no longer requires children’s mental health treatment providers to utilize the Child & Adolescent Service Intensity Instrument (CASII) or Early Childhood Service Intensity Instrument (ECSII) The CASII or ECSII remain useful assessments.
Lacking a better tool for determination of eligibility for CTSS, use the CASII or ECSII as a part of the Child DA to determine Level of Care. A service level rating of 3 or higher justifies CTSS.
Strengths and Difficulties Questionnaire
The Strengths and Difficulties Questionnaire (SDQ) is no longer required, but is an optional measure that may be helpful in some circumstances.The SDQ, asks the child's parents/caregivers, teachers, and children 11 years and older about their behavior and functioning.
Treatment Planning
Use the Child Intake Assessment and Plan for all new admissions.
Use the Integrated Child Service Plan for assembling subsequent CTSS Treatment Plans.
Either plan can be used for any combination of the following services:
- Behavioral Health Home Services
- CTSS Psychotherapy
- CTSS Skills Training
- CTSS Behavior Aide Services
- Child Pyschotherapy*
*Child Psychotherapy is differentiated from CTSS Psychotherapy and is intended for children who are not CTSS-eligible.
Write goals and objectives using those tools, and make sure all goals and objectives you intend to put in the plan are approved. (CTSS Psychotherapy Goals and Objectives are developed in the CTSS service category, no longer in Child Pscychotherapy.)
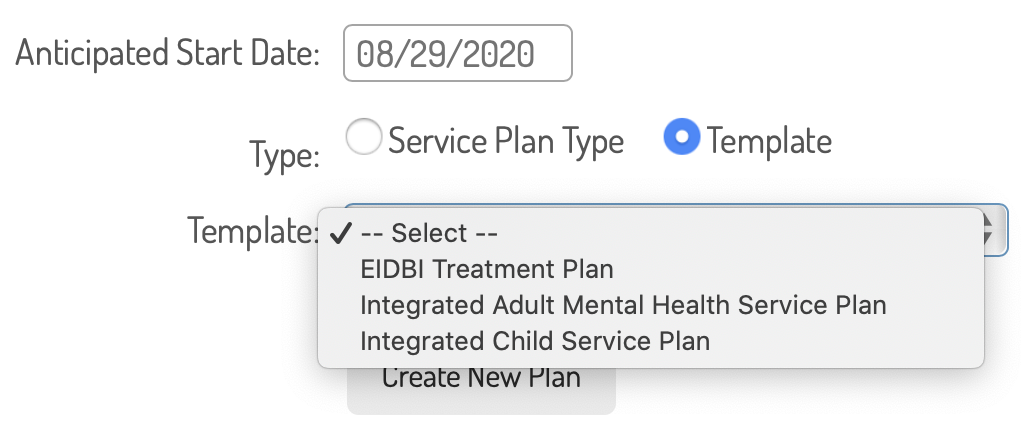
To build the plan, navigate in the child's file to plan and review services > service plans. Enter an anticipated start date and then choose Template and then Integrated Child Service Plan.
Treatment Domains in CTSS
Domains for treatment in the CTSS Plan are:
- Behavioral/Sensory Regulation
- Challenging Behavior
- Developmental Skills for Children
- Interpersonal Functioning
- Parenting Skills
- Psychosocial Skills
- Social and Emotional Competence
- Symptom Management
Requirements and Deadlines for CTSS Assessment and Planning
| Requirement |
Required Item |
Admission Requirement |
Update Required |
| Diagnostic Assessment |
Internal Standard or
Review of External DA |
One year or less prior to admission |
Reviewed annually and a new DA conducted if identified by the conclusions of the review. |
| Treatment Plan |
Tabs Treatment Plan |
Prior to admission |
Every 6 months if reviewed every 2 months, and the review recommendation is to continue the plan as written. |
| Progress Review |
Integrated Child Service Plan Review |
None |
Every 90 days. |
What do CTSS Skills Training Look Like?
CTSS services should be characterized by practice and repitition of skills identified in the treatment plan and CTSS progress notes should reflect this.
As described in the MCHP Manual: Unlike a thought, feeling or perception, a skill is observable by others. It is an activity that must be practiced in order to be mastered and maintained. There are right ways and wrong ways to perform the skill. Typically, a skill is performed for a reason and a skill can be generalized and adapted to many different situations.
As such, using the specific resources, skills, techniques and methods in the Individual Treatment Plan, CTSS Behavior Aides and Practitioners identify the specific skills taught during the session, the child's response and success in demonstrating the skill.
Interventions during the CTSS session include: demonstrating or modeling a skill, prompting a child to complete a skill, providing feedback or correction on the skill, praising effort accomplishment. Avoid interventions during CTSS charactarized by exploring or processing feelings (although emotion-identification can be a skill), advising or coaching on relationships (although teaching a specific communication skill is appropriate), or other activities that resemble talk therapy.
What is CTSS Crisis Asistance?
Provide crisis assistance with prior approval from your Treatment Supervisor, Team Lead, or the Program Director. Crisis assistance is for the child, the child’s family and all providers of services to the child to:
- Recognize factors precipitating a mental health crisis
- Identify behaviors related to the crisis
- Be informed of available resources to resolve the crisis
Crisis assistance requires the development of a written plan that addresses prevention and intervention strategies in a potential crisis, including plans for:
- Actions the family should be prepared to take to resolve or stabilize a crisis
- Arranging admission to acute care hospital inpatient treatment
- Crisis placement
- Community resources for follow-up
- Emotional support to the family during crisis

Assessment and Planning Activities
This work is to be done by mental health professionals and clinical trainees only.
| Service Name |
Description of Activity |
Target Time |
| CTSS Standardized Outcome Measurement |
Activities associated with administering the CASII and ECSII if administered not associated with a Diagnostic Assessment. (Rare).
|
Yes |
| CTSS Treatment Planning |
All treatment planning work completed in interviews or observation of children and/or their parents, Progress Review, and Treatment Plan writeup. Limit is 24 sessions per year. |
Yes |
Child Psychotherapy
CTSS Pscyhotherapy is found in the separate "CTSS Psychotherapy" category. Use the folowing service types for child psychotherapy.
|
Service Name |
Use for |
Target Time
|
|---|
Psychotherapy CTSS
Psychotherapy EL Trainee CTSS |
All sessions. Tabs will determine the billing rate from the duration.
|
Yes
|
|
Psychoeducation Family |
Providing Psychoeducation Services as defined above to family members. Use meeting type to identify if child was present. |
Yes
|
|
Psychotherapy Crisis Child
|
Crisis psychotherapy as defined above.
|
Yes
|
| Family Psychotherapy CTSS |
Family psychotherapy
|
Yes
|
|
Psychotherapy Group Child
|
Group psychotherapy
|
Yes
|
|
Psychotherapy Multi Family Child
|
Group psychotherapy to families
|
Yes
|
Child Psychotherapy Add-Ons
Use the folowing service types for add-ons to child psychotherapy.
| Service Name |
Use For
|
Target Time
|
|
Psychotherapy Child Int Complexity
|
Interactive complexity as defined in the Psychotherapy Guide.
|
No
|
| Psychotherapy Crisis Extended Child |
Extending a crisis therapy session by 30 minutes or more. Two extensions allowed. |
Yes |
|
Therapy Travel Child
|
Travel to a therapy session in a home or community-based setting.
|
Yes
|
Skills Training and Behavioral Aide Services
Use the following service types to document CTSS Skills Training and Behavioral Aide services:
| Service Name |
Use for: |
Target Time |
|
CTSS Crisis Assistance
|
Face-to-face work with children, their parents and family members to develop a crisis plan.
|
Yes
|
|
CTSS Family Skills Training
|
Face-to-face skills training with a child and family members, implementing a Family Skills Training objective from the child's Treatment Plan.
|
Yes
|
|
CTSS in Hospital or Facility
|
Face-to-face skills training with a child who is in a hospital or facility. *This is rare and requires prior-authorization.
|
Yes
|
|
CTSS Skills Training
|
Direct treatment services provided by a Mental Health Practitioner
|
Yes
|
|
CTSS Skills Training Group
|
Direct treatment services provided by a Mental Health Practitioner in a group setting of 3 to 8 children
|
Yes
|
Other Miscellaneous Services and Notes (For Use by All Providers)
| Service Name |
Use for: |
Target Time |
|---|
|
CTSS - Cancellation By Provider
|
Cancellation of a CTSS service by the provider staff.
|
No
|
|
CTSS Client Initiated Cancellation
|
Cancellation of or no-show for a CTSS service by a child or parent
|
No
|
| Therapy Child CCN Travel |
Travel to a cancelled therapy session in a home or community-based setting. |
No |
|
CTSS Contact and Scheduling
|
Calling or communicating with children or parents to arrange services/appointments
|
No
|
|
CTSS File Note
|
Making a note in a child's file
|
No
|
|
Insurance Advocacy
|
Assisting parents in maintaining health care insurance coverage for children.
|
No
|
|
CTSS Service Coordination
|
Coordination of treatment activities, including communicating with other providers of services to the child or parent/family by telephone, face-to-face, or or written communicaiton.
|
No
|
Overall Quality Outcomes of CTSS Services
Overall quality in CTSS services is measured by these broad outcomes:
- Children stay in the family home where behavior or other factors threatened familiy separation
- Children stay in school/make academic progress where behavior or other factors threatened school placement or progress
- Children exhibit reduced symptoms (anxiety, withdrawal, trauma, acting out, etc.) or exhibit coping skills to respond to symptoms
- Children meet development milestones
- Children demonstrate improved psychosocial skills
- Parents, caregivers, teachers, siblings report improved behavior or relationships
Progress Defined
Progress in CTSS services is defined as any of the following:
- Measurable progress or progress reported toward goals identified in the treatment plan
- Progress toward tangible measurable skill development as defined by the treatment plan objectives, based on a progress review
- Improved ratings on a CASII/ECSII as defined by a reduced service intensity rating
- Other, perhaps unexpected progress or improvements in behavior or relationships as reported by the child, a parent, caregiver or teacher
Progress Review
Per Mn Statute 245I: Every two months, a mental health professional must complete a case review of each client assigned to the mental health professional when the client is receiving clinical services from a mental health practitioner or clinical trainee. The case review must include a consultation process that thoroughly examines the client's condition and treatment, including: (1) a review of the client's reason for seeking treatment, diagnoses and assessments, and the individual treatment plan; (2) a review of the appropriateness, duration, and outcome of treatment provided to the client; and (3) treatment recommendations.
Our method to ensure quality, and compliance with this requirement is that Progress Reviews shall be required every two months. Provider staff shall complete a Progress Review that includes:
- an examination of quantifiable data collected during sessions;
- results of interviews with parents and/or children;
- a description of qualitative progress (progress made that is not necessarily measured in outcome statements);
- other relevant information.
The supervising mental health professional will review and approve the Progress Review and discuss the case as necessary, or recommend changes to the plan, methods, etc. and an update to the Plan as necessary.
Updates to the Treatment Plan
CTSS treatment plans must be updated every six months or more often as determined necessary by the Progress Review. Updates must be based upon a review of progress on the previous plan. Where a child has made progress, but has not acheived the targets identified in the previous plan, it is acceptable to continue these objectives into the subsequent plan. Each time required assessments (Diagnostic, SDQ, or CASII/.ECSII are updated, consider the results of these assessments in the plan update as well.
Where a child has not made progress on the defined target outcomes in a previous plan, review the factors that may be impeding progress. These might include:
- Are the techniques and methods the best for teaching the skills? Have they been implemented correctly and consistently?
- Is the relationship between the provider and child effective and therapeutic?
- Have other external factors, such as changes in family or environment, significant life events, or others, impeded progress?
- Has the child made progress in other, unexpected areas that were not measured by the previous plan?
Make modifications to the plan to respond to any of the above.

Adminstrative Discharge
Administrative discharge from CTSS services should occur when:
- A child moves out of the state or to an area within the state where we do not have capacity provide services. If the move is planned, providers should assist the family with and coordinate a transfer to a provider of similar services in the new home.
- A child/family consistently fails to participate in services.
- The child is determined no longer eligible for CTSS because he or she begins to recieve other services that are duplicative of CTSS.
- The child/family chooses to terminate or transfer services.
- The child becomes irreparably uninsured for CTSS and the family cannot or chooses not to pay privately for the service.
Clinical Discharge
Clinical discharge from CTSS services should occur when:
- The update to the Diagnostic Assessment determines that CTSS are no longer medically necessary.
- The supervising mental health professional determines using some metric other than the DA that CTSS are no longer medically necessary.
- The child and/or parent or caregiver decides, in consultation with the supervising mental health professional to end or suspend services.
- The mental health professional, in consultation with the child and/or parents determine that CTSS are not the most appropriate service at this time and a referral is made to the appropriate service.
- Because of various other reasons, CTSS are not resulting in measurable treatment progress, efforts that have been made to modify the plan, techniques, methods, or other impeding circumstances have been attempted, and it is unlikely that continuing services are likely to result in progress.
Discharge Process
Follow these steps for all discharges:
- Complete a final discharge review, noting the reasons for discharge, cosigned by the supervision mental health professional.
- Meet with the family to make recommendations for and referrals to any other needed services and offer support with the transition. Document these in a final File or Service Coordination note.
- Change the child's status for CTSS in TabsTM to Previous, and identify the reason for discharge.
This guide is a living document. We want to improve it with your help. Do you have questions? Found a typo? Find yourself wanting more information? Please send us your thoughts about anything in this chapter by tapping on the link below.
MCHP Manual: CTSS
Mn Statute 245I
Updates to this chapter since July 1, 2022 are listed below.
May 29, 2023:
SDQ clarified as an optional assessment.
Progress Review requirements updated to match 245I.
Resource added: link to Mn Statute 2451.
August 23, 2023:
Clarification of service types to use while documenting CTSS services, including Psychotherapy and Treatment Planning.
January 29, 2024:
Language added to use the CASII/ECSII during the child DA to determine eligiblity for CTSS even if not required by DHS rules. No standard level of care assessment currently exists, so this tool is required by our policy and by some MCOs.
July 11, 2024:
Information about Treatment Domains modified to include Independent Living Skills for Childrenand the callout that DHS does not allow skills for developmental needs (Life Skills) has been eliminated as identified in the Uniform Service Standards Work Group minutes from 4/17/24.
October 2, 2024:
Change in wording regarding Functional Behavior Assessment as a useful tool in treatment planning and reference to the Functional Behavior Assessment for CTSS Skills added.
October 7, 2024: Added wording on the definition of Skills Training