In this section, you will learn about high quality assessment for mental health and behavioral health services. Assessment and planning is not a compliance exercise. Rather high quality assessment and planning that is person-centered, strengths-based, and recovery-oriented is key to success in our work with the people we serve.
This section of the training guide is under construction. Please visit again soon to see our progress.
Principles of Assessment and Planning
Assessment and Planning for Mental Health services is a meaningful, ongoing process that helps identify an individual's recovery goals, current strengths and resources, needs, and barriers to recovery, including impairments in functioning. It is charactarized by the following four values.
Strengths-Based
Strengths-based means recognizing and starting treatment with and individual's strengths, not with his or her deficits. As Charles Rapp put it in his 1997 book "The Strengths Model" it is "ampllifying the well." While ARMHS eligibility is defined by deficits, treatment in ARMHS should be charactarized by buillding on an individual's strengths, current resources, and resourcefulness.
Person-Centered
Person-centered means that the people we serve have control over their services, including the amount, duration, and scope of services, and choice of providers. Person-centered services respond to the needs of the individuals served as they have defined them and respect choices. Recipients participate in the development of treatment goals and services provided, to the greatest extent possible.
Most importantly, person-centered services means that we exhibit unconditional positive regard. We accept and embrace occasional ambivalence and, with empathy and compassion, understand undesirable choices and behavior as symptoms of illness.
Models over care changed over time. A traditional/historical model of care focused on the diagnosis, disease, and deficits, where as a person centered model of care focuses on the client’s abilities, preferences, and individual needs. The following table compares the focus of various aspects of the traditional/historical model of care and the person centered model of care. The comparison shows that a person centered model of care recognizes and empowers the individual in treatment.
Historical/Traditional
Person Centered
Deficit-based model of care, using standardized assessments and treatments
Strength-based model of care. Disability is only one of the characteristics considered in model of care.
Care is focused on fixing problems.
Care is focused on supporting the in learning skills.
Professionals make decisions about treatment
The client makes decisions about care.
Control: professional judgement and decision making
Partnership/shared decision making
Goals decided for the client
Driven by the individual's goals
Stabilization is the desired result
Quality of life is the desired result
Fit person and treatment plan into the program parameters
Individualized
When talking or writing about a client it is important to use person centered language. Using person centered language paints the client in a positive light. When talking about a person ensure that you:
> Refer to the client by name as opposed to by case > Refer to a positive UA as a 'positive UA' as opposed to a 'dirty UA' > Describe the client as assuring needs are met as opposed to manipulative > Describe the client as pre-contemplating change as opposed to in denial > Describe the client as reluctant and cautious as opposed to resistent > Refer to the care coordinator as the care coordinator as opposed to the case manager
When writing a Recovery Oriented Plan include the following:
> Avoid jargon > Identify a person's strengths > Make evident what and who is important to the person > Ensure that the purpose and goals of the plan are connected to the persons hopes and preferences > Know how to best support the person to acieve what is important to him/her in a balanced way > Ensure the recovery plan is centered on the person's recovery goals and vision
One page profiles lead to positive change for a person by listing what really matters for that person. In a single page, a One Page Profile embodies significant information about a person. The three headings in a One Page Profile are: what people appreciate about me, what’s important to me and how best to support me. Answering these questions in one page provides a foundation for relationship building, ease in transitioning from service to service, and reflect changing circumstances when updatingn the profile. The following video reflects the outcome of using a One Page Profile.
Recovery-Focused
For a working definition of recovery from SAMHSA, the Substance Abuse and Mental Health Services Administration read this article now. It is this definition around which we have developed our treatment model at Accend.
Goal-Oriented
Goals are positive, desired outcomes we are striving toward, not undesired current or previous conditions we are trying to avoid. In goal-oriented services, we help each individual we serve identify their wants, and needs, goals, hopes and dreams, form these into positive goals and then go about making a plan to achieve them. And we measure success as progress toward these goals.
Diagnostic Assessment
What You Will Learn
Use a Diagnostic Assessment to...
Purpose
All mental health/behavioral health services begin with A Diagnostic Assessment, or DA. A DA is conducted by a licensed Mental Health Professional or Clinical Trainee and serves these core purposes:
to identify whether or not a referred individual has a diagnosis (or diagnoses) of mental illness or a behavioral disorder;
to identify the diagnoses and their severity;
to preliminarily determine a referred individual's eligibility for services;
to make recommendations for services based on the individuals diagnoses and the needs the person has identified in the DA and Intake interviews; and
in the case of an annual DA update, one of several strategies we use to assess treatment progress and success..
DA Requirements and Deadlines
A DA is required prior to admission and annually for continuing all community-based mental health services. To establish intitial and continuing eligibiilty, the DA must identify a mental health or behavioral disorder, and for services other than pscyhotherapy, determine that services are medically necessary due to impairments in functioning or risks of harm, hospitalization or residential treatment resulting from the idnvidual's diagnosis, symptoms and/or behavior.
Find additional requirements for eligibility for each of the different services we provide in the guide section for those specific services.
A Diagnostic Assessment is complete after it all of the findings and treatement recommendations have been written and it has been approved by a Licensed Mental Health Professional.
Types of DAs
There are two basic types of Diagnostic Assessments. These are:
The Brief DA
Used rarely, the Brief DA consists of an interview and write-up, but includes less information than a standard DA. A breif DA might be appropriate for an individual who will not likely need more that 10 total sessions of any kind of mental health treatment following the DA.
The Standard DA
Used most often, the standard DA consists of an interview and write-up.
The Review of Previous DA
Annually, the previous Diagnostic Assessment needs to be reviewed, and updated as determined by that review. See procedures and requirements for the Review of Previous DA here.
Explanation of Findings
Explanation of Findings is a service that can follow a DA that consists of meeting with a person who has received a Diagnostic Assessment, and perhaps family members or service providers, to explain the diagnosis, findings, and treatment recommendations in the DA.
Learn More
Tap on the following links to learn more about DAs and Explanation of Findings in the Minnesota Health Care Program (MHCP) manual
Along with the DA, the Functional Assessment is the core document used for identifying:
What You Will Learn
Use a Functional Assessment to...
Basic needs
Current strengths and resources for acheiving goals and recovery vision
Barriers to goals and recovery
Current functioninng and impairments in functioning
Links between mental health symptoms and impairments in functioning
Strategies and priorities for mental health services and treatment
Progress on all of the above (in subsequent FA updates)
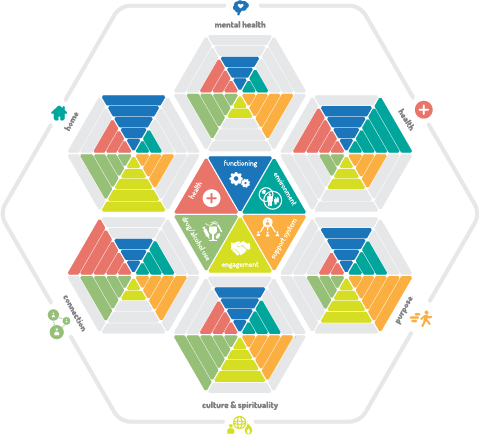
What is 6X6 Functional Assessment?
At Accend, we call our Functional Assessment the 6X6 FA. It is designed from the lessons we have learned in our many years providing adult mental health services, and around the SAMHSA definition of recovery you read about above. What is 6X6?
Six Domains of Recovery
1. Mental Health: While the SAMHSA definition defines mental health and health together as one of four elements of recovery, in our FA, we assess mental health symptom identification and management separately, while understanding the vital links between mental and physical health.
2. Health: Both impacted by and impacting mental health, physical health, including good health habits, nutrition, exercise, and obtaining and using health and dental care is a core element of recovery.
3. Home: The Home domain includes skills and resources for independent living, including activities of daily living, obtaining and maintaining housing, managing finances, and transportation.
4. Connection: Connection includes relationships with family, friends, neighbors, and effective interpersonal communication and self-advocacy skills with these, and with service and support professionals, landlords, and others.
5. Purpose: Purpose examines work, education and civic and community involvement. Important to understand is that purpose is defined differently for everyone, and can include many different "meaningful daily activities, such as a job, school volunteerism, family caretaking, or creative endeavors, and the independence, income, and resources to participate in society."
6. Culture and Spirituality: For some, culture and spirituality is an extension of Purpose. In their cultural and spiritual practices and beliefs, they find meaning and purpose. For some, culture and spirituality provides Connection to others and identity that grounds them. And for some, culture and spirituality informs Health care decisions, or is a core element of healing and recovery.
Finally, for some, culture and spiritual beliefs and practices from their past may complicate their recovery process as they redefine their belief systems or adapt to new or evolving cultural values or experience a process of social, psychological and cultural change through the blending of past and new cultural norms and values in a process called acculturation. While we do not provide treatment directly addressing this domain, understanding and respecting an indvidual's cultural and spiritual belief systems can inform and improve treatment in other domains.
Six Axes of Progress
1. Functioning: Improving functioning where it is impaired by the symptoms of mental health is a core element of the community-based mental health services of Case Management and Adult Rehabilitative Mental Health Services. The 6X6 FA examines functioning in each domain and identifies how it is impacted by, or impacts mental health symptoms.
2. Environment: For some, impairments in functioning are a condition of an environment that is not safe, stable, or supportive. For others, where impairments in functioning are chronic, impacts of these impairments can be lessened, or accommodated by a supportive environment. In either case, rehabilitative services and case management can help individuals identify and make changes in their home, work, school and social environments that are supportive and optimal for them.
3. Support Network: An individual's Support Network includes natural, or informal supports like family, friends, neighbors, and community members, and paid professionals in health and mental health care, residential, vocational, educational, financial, social services and other fields. Assessing an individuals support network, and connecting individuals with support systems can for many, be a core and vital lelement of recovery.
4. Health: Where health conditions impact, or are impacted by, functioning or symptoms, assessment of these impacts, and treatment targeted at reducing either is another core element of recovery. And, where a health condition or physical disabillity is the primary cause of impairment in functioning, the case manager or rehabilitation practitioner can assess an individual's Environment and use of his or her Support Network and resources as a possible focus of treatment.
5. Substance Use: Substance Use can often be a form of self-medication, albeit one that is not conducive to recovery. Substance abuse or dependency can be a powerful barrier to recovery. Where abuse or dependency is a barrier, treatment might emphasize symptom management and healthy habits as an alternative to self-medicating with drugs or alcohol, and connecting with supports and resources to treat the abuse or dependency problem.
6. Engagement: Engagement measures an individuals readiness for change and participation in medically-necessary services and supports. It describes a persons progess moving from a place of ambivalence to partnering with providers and setting and accomplishing recovery goals.
Conducting the Functional Assesment
Rather than a one-time-every-six-months event, Functional Assessment is an ongoing process, integral to treatment, and one that provides benchmark measures of treatment success. Functional Assessment can and should, wherever possible, take place in context, while doing with, rather than
Service Intensity Assessments for Children
Service Intensity (Level of Care) Asssessments are no longer required for adult (ARMHS and Case Management) services.
CASII and ECSII
The CASII and ECSII are equivalent level of care instruments for children. While no longer required by DHS rules or statutes, these are required by Accend policy, also due on admission and updated with each new DA.
Treatment Planning
Elements of Treatment Plans
Treatment Rationale
For Treatment Plans for services that require a Functional Assessment or Health and Wellness Assessment (FA/HWA), the treatment rationale populates from this assessment. It will not auto-populate until the most recent FA/HWA is approved. Make sure you are completing these documents in the proper order. It is fine to begin writing objectives before the FA/HWA is done, but once that is completed, refreshing the data in each treatment objective will pull that information into it.
Treatment Rationale is included here because it is the all-important why is treatment needed here, and established medical necessity. While completing the FA/HWA, keep this in mind.
For objectives where the service does not require a FA/HWA, you will be required to write the treatment rationale in the objective utility.
Goals
Goals are the client's. These not be as specifically measurable as outcome statements but should reflect the client's desire for change in a general, or a specific sense.
Objectives
Objectives are tied to the domains where the client wants to make changes related to a specific goal. In this utility, choose the goal to which the objective is tied.
Outcomes
Outcomes are the measurable and crucial element of each Treatment Objective.They describe the observable or reportable results of treatment/services. These are how we measure success in the Progress Review. Outcome statements should be Meaningful, Measurable, and Achievable. The exercise below explores that.
There is more to come in this section. Send feedback and suggestions at the link below.
Feedback or Questions about this Chapter
This guide is a living document. We want to improve it with your help. Do you have questions? Found a typo? Find yourself wanting more information? Please send us your thoughts about anything in this chapter by tapping on the link below.